The soleus muscle plays a critical yet often underestimated role in lower limb performance and injury. Composed of approximately 80–90% type I muscle fibres, the soleus is uniquely adapted for endurance, postural control, and sustained force production. Type I fibres are slow-twitch, highly fatigue-resistant, and rely predominantly on aerobic metabolism, making them ideal for prolonged, repetitive loading rather than rapid, explosive movements.
During running, the soleus is subjected to enormous demands, experiencing forces estimated at up to 8 to 12 times body weight with each gait cycle. When the capacity of the soleus is exceeded, injury can occur, often with significant implications for running performance and recovery.
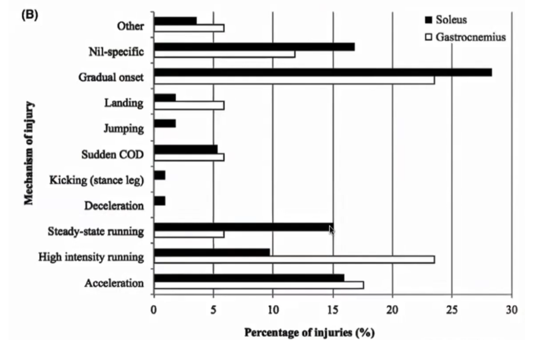
Soleus muscle injuries typically occur when the cumulative load placed on the muscle exceeds its capacity to tolerate sustained force production. Because the soleus is most active during mid-stance and propulsion in running, particularly when the knee is flexed, it is repeatedly required to generate high levels of force for prolonged periods. Factors such as sudden increases in training volume or intensity, hill running, speed work, fatigue, or reduced ankle dorsiflexion can all increase soleus demand. Over time, inadequate recovery or insufficient strength and endurance of the muscle may lead to micro-trauma within the muscle–tendon unit, progressing to pain, stiffness, or strain without a single identifiable traumatic event. See below a table summarizing and comparing the mechanism of injury of the soleus muscle versus the other muscle of the calf complex – gastrocnemius.
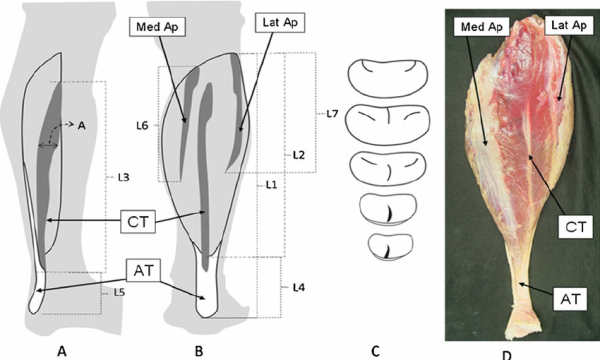
Anatomically, the soleus muscle has several unique features that influence both its function and injury behaviour. Unlike many muscles, the soleus contains a broad, complex intramuscular aponeurosis that runs through its centre (central tendon), providing an extensive surface area for muscle fibre attachment. This structure effectively creates a “muscle within a muscle,” with fibres arranged on either side of the aponeurosis rather than running the full length of the muscle. While this design enhances the soleus ability to generate and transmit large, sustained forces, it also introduces regions of high mechanical stress. As a result, injuries often occur within or adjacent to the aponeurosis itself, contributing to the deep, poorly localised pain and prolonged recovery commonly seen with soleus muscle injuries.
How can Physiotherapy help?
Physiotherapy plays a key role in the management of soleus muscle injuries by addressing both load tolerance and movement strategy. A thorough assessment allows exercises to be specifically prescribed to target the soleus, and the medial or lateral component depending on the injury location. This is commonly achieved by manipulating knee position, ankle range, ankle position, and speed of loading - such as using bent-knee calf raises, isometric holds, or slow heavy resistance exercises. By progressively exposing the injured tissue to the demands it must tolerate, physiotherapy helps restore capacity, reduce re-injury risk, and support a safe return to activity.
At Foundation Clinic, force plate testing is used to objectively guide rehabilitation and decision-making throughout recovery from soleus muscle injury. By assessing key metrics such as peak force, rate of force development, and asymmetry we gain insight into how well the injured soleus is functioning compared to the uninjured side. This data helps inform exercise progressions during rehabilitation and provides clear benchmarks for return to running, return to speed, and ultimately return to sport. Rather than relying solely on symptoms or time-based criteria, force plate testing allows rehabilitation to be individualised and progression to be based on measurable readiness, reducing the risk of re-injury.
For more information book an appointment, or contact [email protected]
References:
Balius, Ramon & Alomar, Xavier & Rodas, Gil & Miguel, Maribel & Pedret, Carles & Dobado, Mari & Blasi, Juan & Koulouris, George. (2012). The soleus muscle: MRI, anatomic and histologic findings in cadavers with clinical correlation of strain injury distribution. Skeletal radiology. 42. 10.1007/s00256-012-1513-3.
Coventry, Molly & Latella, Christopher & Green, Brady & Mosler, Andrea & Peak, Jayden & Armendariz, Maria & Rio, Ebonie & Murphy, Myles & Pérez Armendáriz, Maria Luciana. (2025). Voluntary activation of the ankle plantar flexors: A systematic review and meta-analysis. JSAMS Plus. 6. 10.1016/j.jsampl.2025.100117.
Green, Brady & Lin, Monica & Schache, Anthony & Mcclelland, Jodie & Semciw, Adam & Rotstein, Andrew & Cook, Jill & Pizzari, Tania. (2019). Calf muscle strain injuries in elite Australian Football players: A descriptive epidemiological evaluation. Scandinavian Journal of Medicine & Science in Sports. 30. 10.1111/sms.13552.